NEUROIMAGING / NEUROSONOLOGY
Transcranial Doppler ultrasound
Updated on 11/11/2023, published on 24/10/2023
Trancranial Doppler ultrasound (TCD/TCCD) is a non-invasive imaging technique helpful in evaluating flow in intracranial vessels → general indications for the examination
Transcranial examination procedure
Methods
- the probe utilizes ultrasound with a frequency of 2-2.5 MHz
- in pulse-wave (PW) mode, the device registers the frequency shift (∆f) created by the reflection of ultrasound from moving blood particles and converts it into a graphic record and audible sound using FFT transformation
- transcranial Doppler sonography (TCD) allows measurement of flow (by obtaining the Doppler waveform) in intracranial arteries
- velocities are calculated from the frequency shift of the reflected ultrasound beam,
- TCD displays no anatomical structures; the examined vessel is determined by the insonation depth and probe position
- correction of the insonation angle is not possible (insonation angle is considered to be 0 grade)
- transcranial color-coded Doppler (TCCD)
- TCCD provides enhanced diagnostic capabilities compared to standard TCD
- in addition to Doppler waveform, TCCD integrates B-mode imaging to visualize anatomical structures, as well as color, energy, or B-flow modes for vessel identification
- sample volume can be thus reliably positioned within the desired arterial segment
- angle-corrected flow velocities can be obtained
- these velocities are up to 30% higher than uncorrected velocities obtained on TCD
- limitation: an impenetrable temporal bone window (affecting ~ 5-20% of patients)
- a large proportion of these patients can be investigated using contrast agents (ECHOVIST, SONOVUE)

 with normal waveform in the MCA")
Transcranial windows
TCD/TCCD is typically examined using a high-frequency transducer placed over specific cranial windows (regions where ultrasound imaging can be performed with minimal interference from bone):
- temporal

- horizontal plane: terminal ICA (TICA), segment M1-3, A1-2, P1-2, AComA, PComA
- anterior temporal artery (ATA) can be detected in P2 segment
- anterior coronal plane: better visualization of the terminal ICA

- posterior coronal plane: distal BA, PCA, and possibly SCA
- horizontal plane: terminal ICA (TICA), segment M1-3, A1-2, P1-2, AComA, PComA
- transforaminal (posterior circulation) – V4, BA, potentially PICA, AICA, or SCA)

- transorbital (carotid siphon and ophthalmic artery) – reduce power to 10-15%


- complementary approaches:
- submandibular (distal extracranial ICA segment)

- frontal (A2)
- occipital (dural sinuses, BA+VA)
- submandibular (distal extracranial ICA segment)
- in 5–20% of cases, cranial hyperostosis is the cause of poor insonation window, particularly in the temporal region
- incidence can vary among populations; factors such as age and ethnicity can influence this rate
- even in the absence of a color flow signal, a satisfactory Doppler waveform may sometimes be acquired

- consider the use of echo contrast agents to enhance image quality
- the quality of the bone window is crucial for the sensitivity and specificity of transcranial sonography
| The quality of the temporal bone window can be assessed in five degrees: | |
| absent |
|
| very bad |
|
| bad |
|
| average |
|
| perfect |
|
Examination
Correct evaluation of the Doppler waveform in the examined arteries is crucial; it is essential to take into account the findings in the extracranial arteries and to consider additional factors (hypotension, significant changes in pCO2, arrhythmias, marked anemia, valvular defects, etc.)
- assess the flow pattern (laminar x turbulent)

- evaluate Peak Systolic Velocity (PSV), End Diastolic Velocity (EDV), Resistance Index (RI), and Pulsatility Index (PI), as well as systolic acceleration (acceleration time)
- compare flow on both sides (unless there is pathology there, too) and between individual arteries
- normal findings
- interhemispheric difference < 20-30%
- PSV: MCA > ACA, ACM > PCA, BA > VA
- cut-offs for normal PSV and EDV (see in the table)
- RI < 0.8 and PI < 1.0
- identify possible steal syndrome
- subclavian-vertebral steal

- flow diversion due to arterial occlusion (such as increased ACA flow in case of MCA occlusion; PSV ACA>MCA)

- steal syndrome due to AVM or DAVF
- subclavian-vertebral steal
- search for embolic signals (HITS)

- spontaneous
- provoked as part of a bubble test
- asssess cerebral vasomotor reactivity (CVR) in selected cases
- note other waveform alterations
- arrhythmias (e.g., atrial fibrillation)

- altered flow due to valvular defects or impaired ejection fraction
- arrhythmias (e.g., atrial fibrillation)
Normal finding
- continuous, laminar flow, no aliasing
- normal systolic acceleration (AT)
- normal PSV/EDV and resistance indices (see table below)
- PSV/EDV ± < 2SD
- PI/RI ± < 1SD
- no HITS, no turbulence or low-frequency murmurs
- normal CVR
- no arrhythmias
| Average velocities in cm/s (with angle correction) +- 1 standard deviation (SD) | ||||
| Artery |
flow velocity and resistance index
|
age | ||
| 20 – 40 years |
40 – 60 years | > 60 years | ||
| MCA |
PSV (cm/s)
|
91 -126 | 84 – 120 | 78 – 109 |
| EDV (cm/s) | 37 – 70 | 35 – 61 | 28 – 48 | |
| RI | 0,48-0,59 | 0,47-0,58 | 0,5-0,65 | |
| ACA | PSV (cm/s) | 67-102 | 62-96 | 49-91 |
| EDV (cm/s) | 31-50 | 30-46 | 25-39 | |
| RI | 0,5-0,59 | 0,48-0,57 | 0,51-0,6 | |
| PCA | PSV (cm/s) | 50-78 | 45-73 | 41-73 |
| EDV (cm/s) |
21-37
|
21-35 | 17-31 | |
| RI | 0,48-0,56 | 0,48-0,56 | 0,49-0,66 | |
| VA | PSV (cm/s) | 46-76 | 38-74 | 38-62 |
| EDV (cm/s) | 23-43 |
18-40
|
14-29 | |
|
RI
|
0,44-0,57 | 0,44-0,57 | 0,48-0,63 | |
| BA | PSV (cm/s) | 48-80 | 49-82 | 37-65 |
| EDV (cm/s) | 26-43 | 19-40 | 13-25 | |
|
RI
|
0,46-0,56 | 0,46-0,56 | 0,5-0,62 | |
Assessment of arterial stenosis
- a multiparametric evaluation is necessary; an isolated PSV obtained from the stenotic segment is not sufficient
- obtain PSV, PI, and RI in the stenosis and in the pre-and poststenotic segments (if possible)

- assess PSV ratio and collateral circulation
- obtain PSV, PI, and RI in the stenosis and in the pre-and poststenotic segments (if possible)
- prestenotic segment: a resistant (↑PI and RI) and decreased flow
- stenotic segment:
- turbulent flow with increased PSV
- PVS should be > 30% higher than contralateral (unless stenosis is bilateral)
- PSV ratio (PSV in stenosis / pre- or poststenotic segment) (see table)

- aliasing phenomenon (manifestation of turbulences in color flow mode)
- turbulent flow with increased PSV
- poststenotic segment: decreased PSV, systolic acceleration, PI, and RI
| PSV ratio (stenosis / pre- or poststenotic segment) |
Stenosis (%) |
|
| mild stenosis | 1.3-2 | < 50% |
| moderate stenosis | 2-3 | 50-70% |
| severe stenosis | > 3 | > 70% |
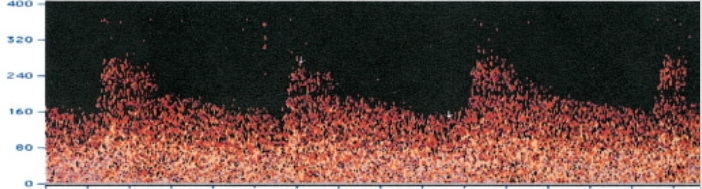
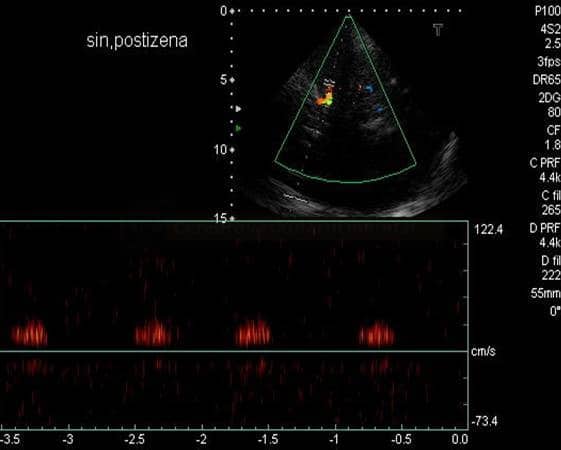
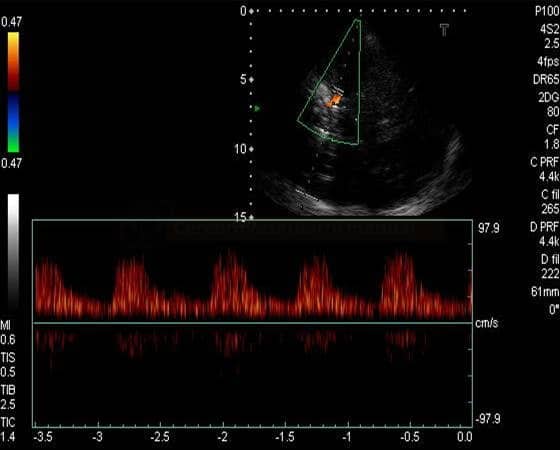
STENOSIS IN M2 SEGMENT OF THE MCA
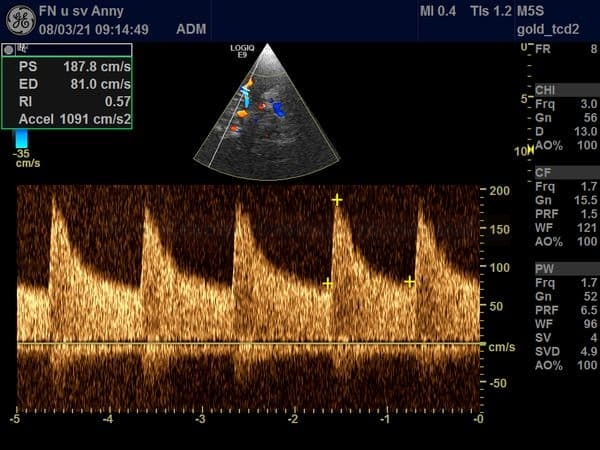 Stenotic turbulent flow at the origin of M2 segment
Stenotic turbulent flow at the origin of M2 segment
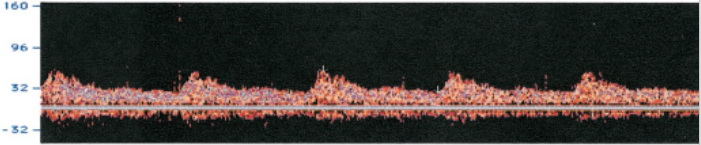
 Flow in proximal M1 segment
Flow in proximal M1 segment
 Flow in distal M2 segment
Flow in distal M2 segment

![]()
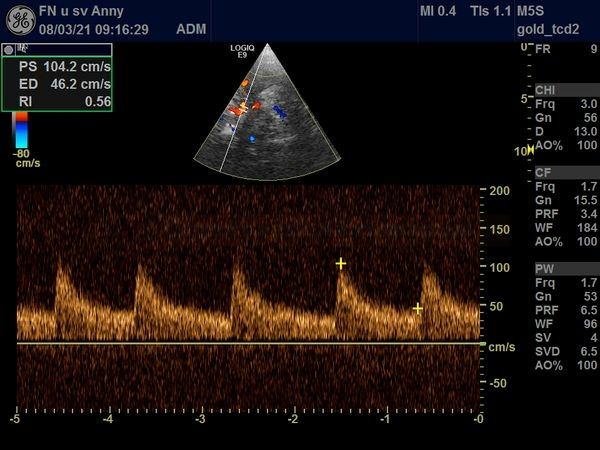
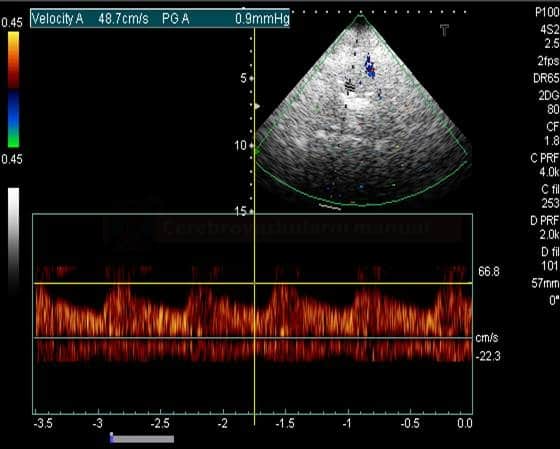
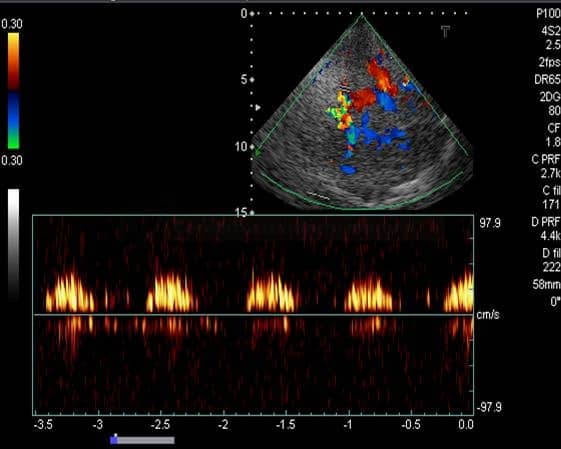
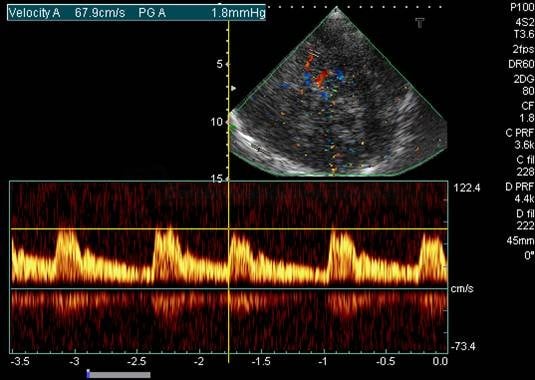
STENOSIS IN THE M1 SEGMENT OF THE MIDDLE CEREBRAL ARTERY
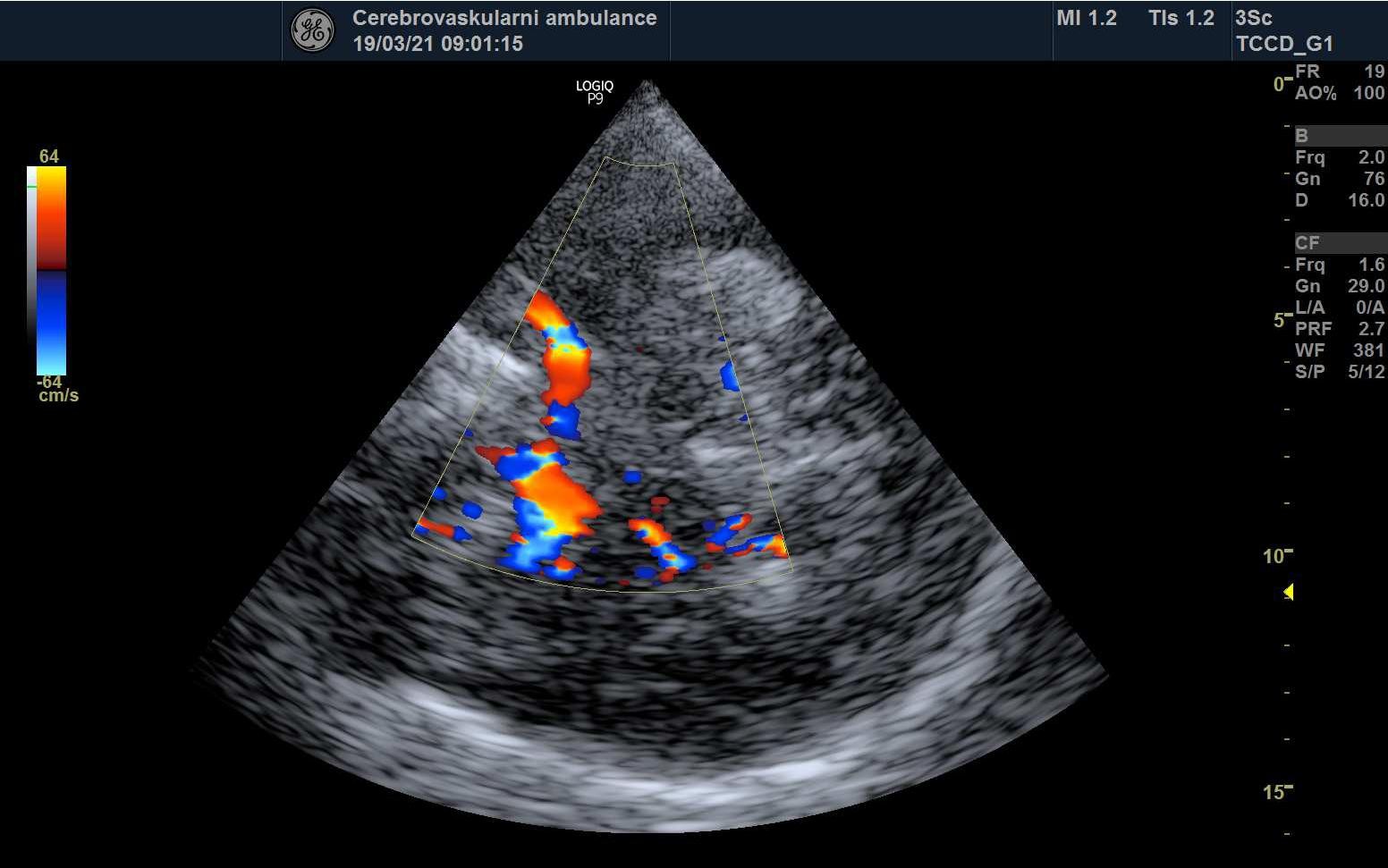 MCA stenosis in color flow mode (CFM) characterized by aliasing
MCA stenosis in color flow mode (CFM) characterized by aliasing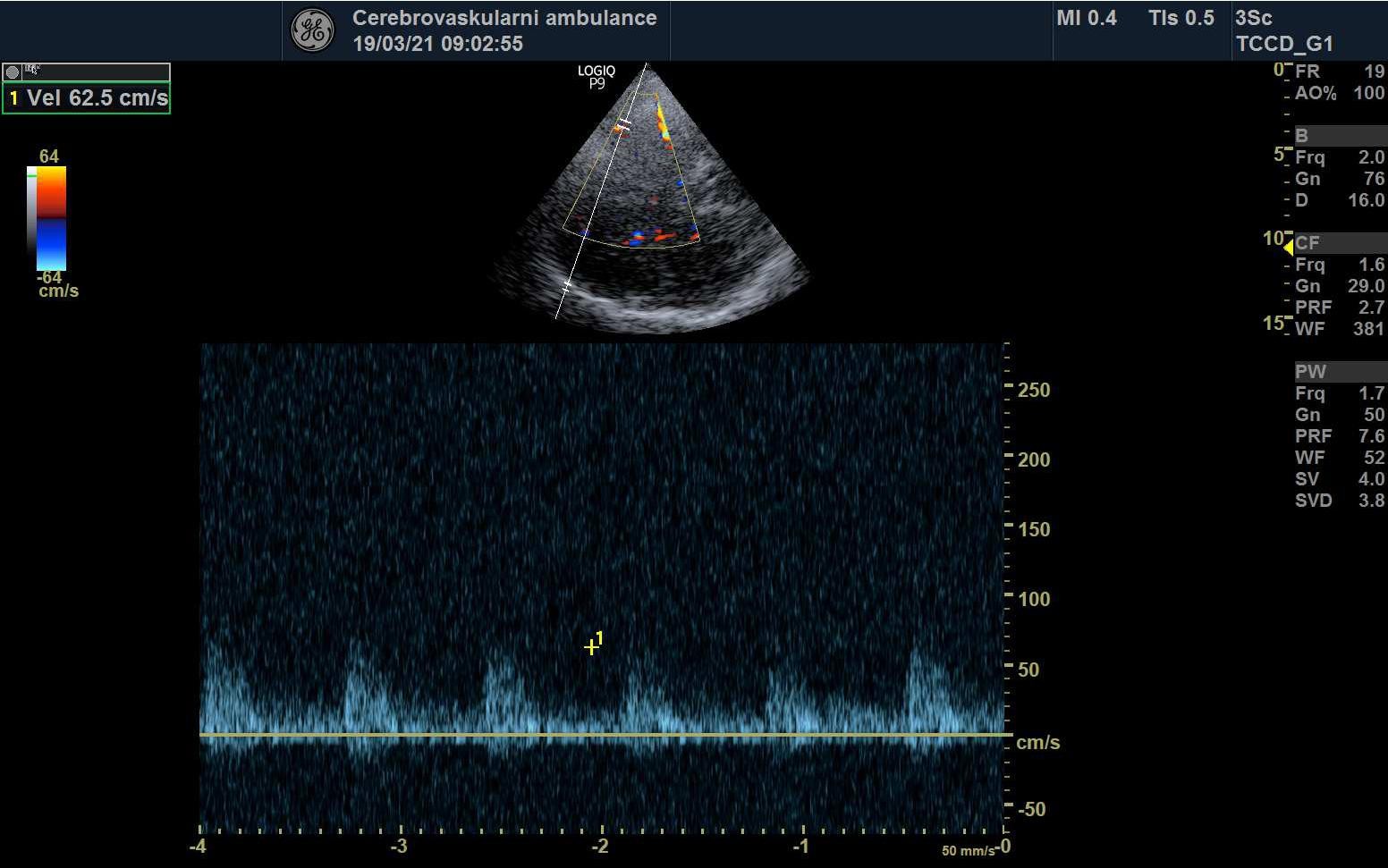 Poststenotic flow in M2 segment
Poststenotic flow in M2 segment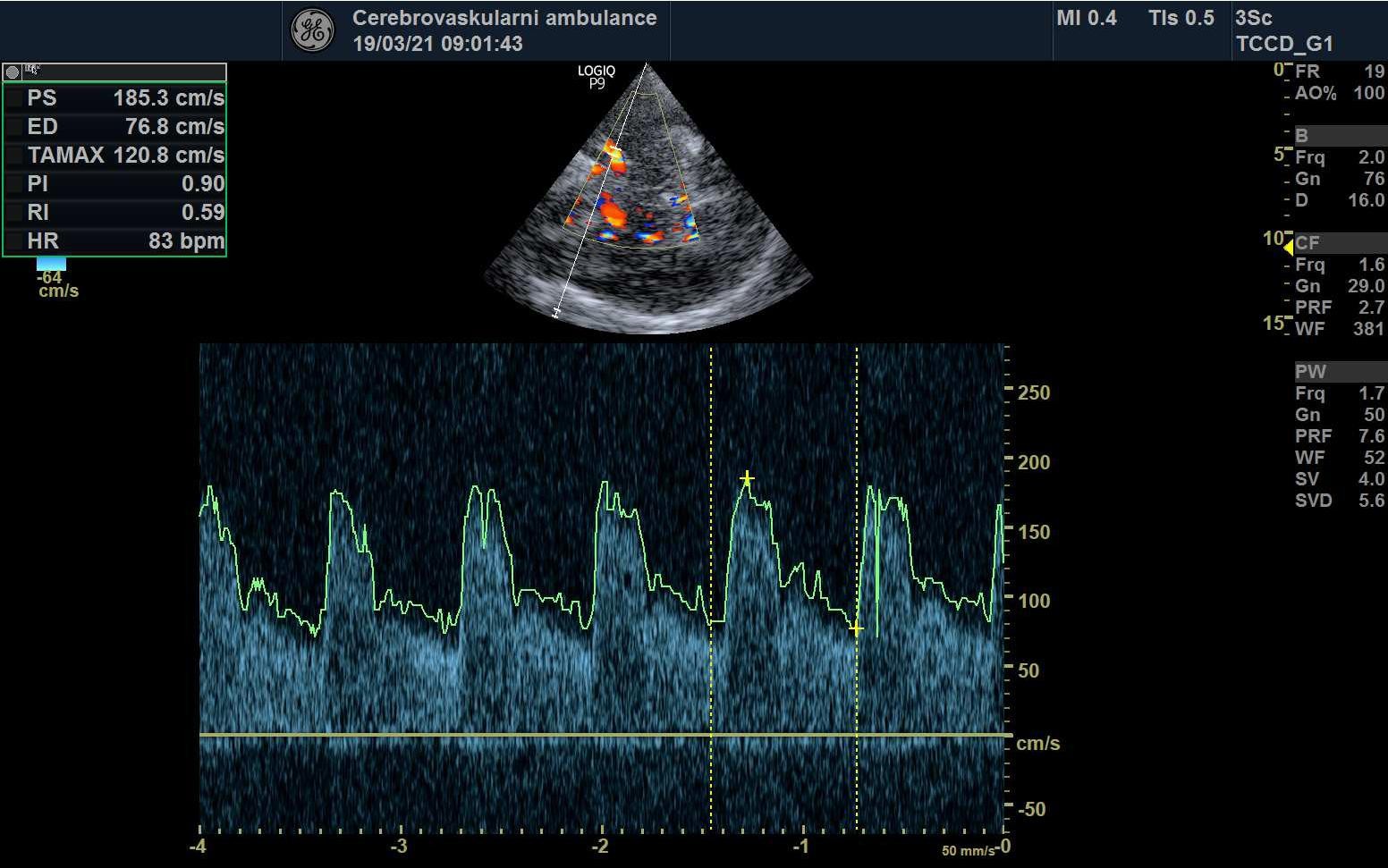 Turbulent flows at the stenosis segment with PSV 185/76 cm/s. The PSV ratio (stenotic/prestenotic segment) is 3, corresponding to a stenosis near 70%
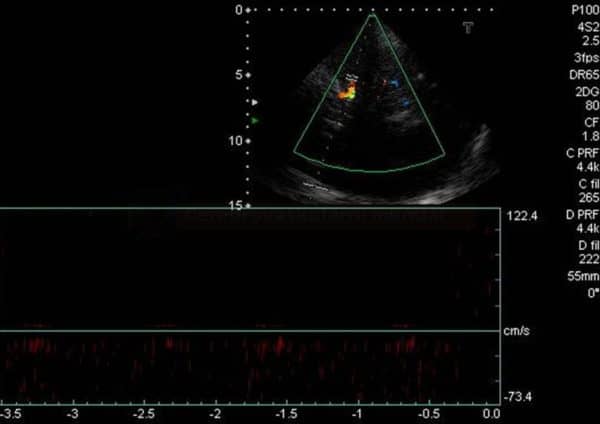
Turbulent flows at the stenosis segment with PSV 185/76 cm/s. The PSV ratio (stenotic/prestenotic segment) is 3, corresponding to a stenosis near 70%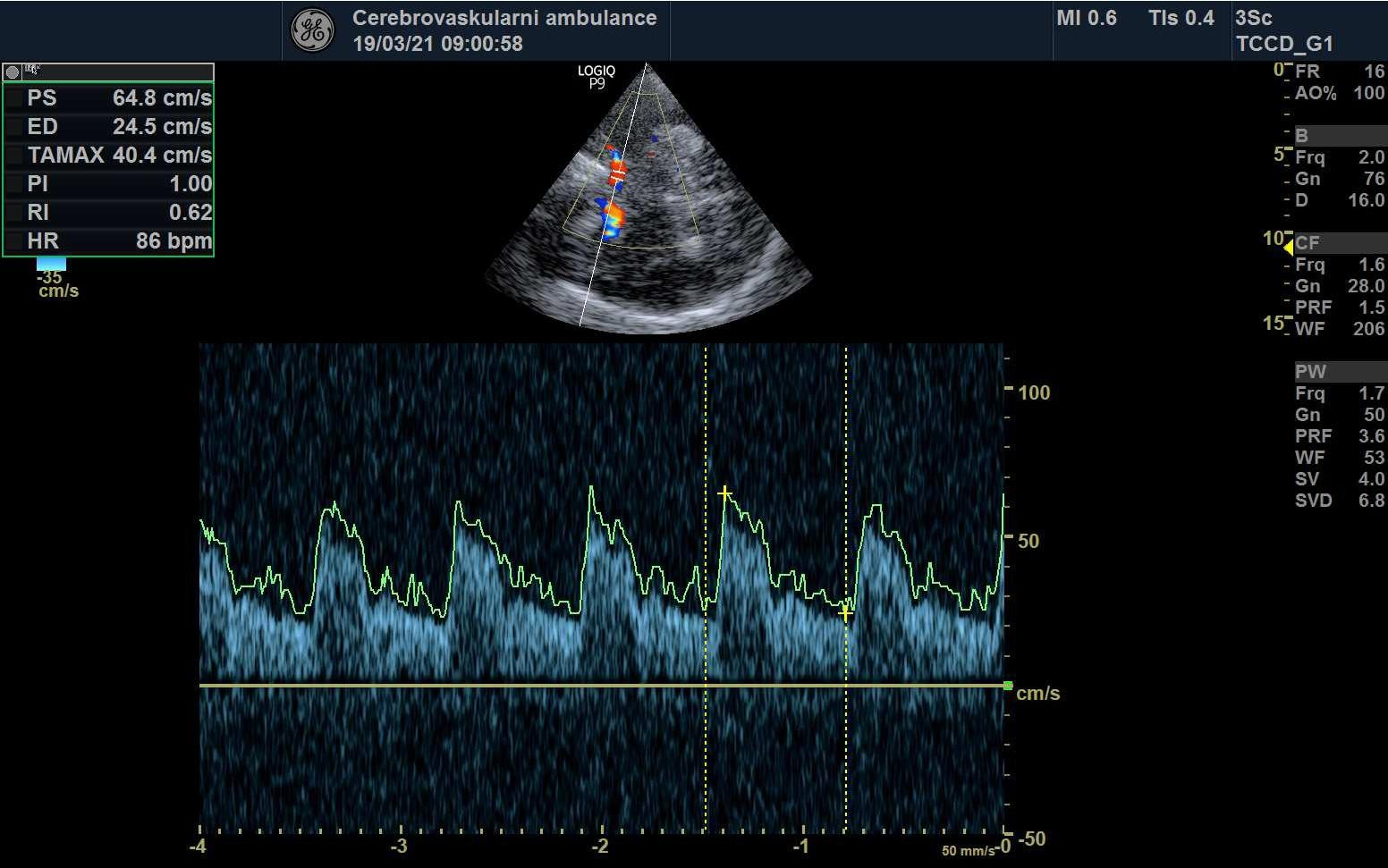 Flow in the proximal MCA (prestenotic segment)
Flow in the proximal MCA (prestenotic segment)
![]()
Assessment of arterial occlusion
- transcranial Doppler (TCD or TCCD) is an ideal noninvasive, real-time bedside tool for the evaluation of cerebral vessels, particularly in the setting of an acute stroke
- strong correlation exists between TCCD and CTA
- an abnormal TCD/TCCD study, defined as either no or asymmetrical MCA flow, is associated with poor outcome
- direct signs of occlusion:
- absence of the artery in color mode with good visualization of other arteries (or veins)
- absent or altered flow (TIBI/COGIF criteria)
- indirect signs:
- decreased PSV and increased PI and RI proximal to the occlusion
- with M1 or multiple M2 branches occlusion, flow diversion can be detected ( PSVACA > PSVMCA)
- assessment of basilar artery occlusion (BAO), especially of its distal segment, may be challenging
- due to numerous branches, the findings in the proximal segments may appear practically normal
- the patency of the distal BA can be verified by inducing undulations in the PCA by tapping the extracranial VA (usually behind the ear)

TIBI (Thrombolysis in Brain Ischemia)
- the TIBI classification was developed to grade residual flow
- it correlates with initial stroke severity, clinical recovery, and mortality in acute stroke patients
- no improvement in the residual flow correlates with the absence of early clinical recovery and increased mortality (Demchuk, 2012)
- no improvement in the residual flow correlates with the absence of early clinical recovery and increased mortality (Demchuk, 2012)
 |
TIBI 0 – absent flow
– lack of regular pulsatile flow signals despite varying degrees of background noise
|
 |
TIBI 1 – minimal flow
– systolic spikes of variable velocity and duration
– EDV = 0
– possible reverberating flow
|
 |
TIBI 2 – blunted flow
– flattened systolic flow acceleration of variable duration compared to control side
– PI < 1,2 – positive EDV |
 |
TIBI 3 – dampened flow
– normal systolic flow acceleration
– positive EDV – decreased flow (MFV) by > 30% compared to the control (healthy) side
|
 |
TIBI 4 – stenotic flow
– MFV > 80cm/s + velocity difference (MFV) of > 30% compared to the control side (increased velocity)
– turbulence + velocity difference (MFV) of > 30% compared to the control side (increased velocity) |
 |
TIBI 5 – normal flow – symmetrical flow or < 30% MFV difference compared to the control side |
According to [Demchuk, 2001]
| Recanalization assessment [Clotbust, 2007] |
|
| Complete recanalization | TIBI 4-5 |
| Parcial recanalization | increase of TIBI by ≥1 grade (but not to 4 or 5) |
| Reocclusion | decrease of TIBI by ≤1 grade |

COGIF
Differentiation of TIBI grades 1-3 (minimal flow, blunted flow, dampened flow) may be difficult. The flow patterns of these grades not only reflect partial M1 recanalization but also the hemodynamic situation in other segments. The COGIF scoring system was designed to more clearly follow the recanalization process; it is exclusively based on known hemodynamic changes of the Doppler spectrum. The time course of grades during the serial examination must be encoded.
|
COGIF GRADE (Consensus On Grading Intracranial Flow obstruction)
|
||
 |
COGIF 1
– no flow |
|
  |
COGIF 2
– low flow
– EDV = 0
|
|
 |
COGIF 3
– low flow
– EDV > 0 |
|
  |
COGIF 4
4a – normal (symmetrical flow) 4b – focal flow acceleration (probable stenosis)
4c – high segmental flow (hypercirculation)
|
|
| Recanalization assessment | |
| Complete recanalization |
COGIF 4 |
| Partial recanalization |
improvement by ≥1 grade (but not to 4) |
| No change |
baseline COGIF grade persists |
| Worsening | decrease by ≥1 grade |
Transcranial findings in extracranial stenosis/occlusion
- ↓PSV and EDV
- ↓ PI, RI
- decreased systolic acceleration
- development of collateral circulation
- retrograde flow in the ophthalmic artery (OA)
- retrograde flow in the ipsilateral ACA
- well-marked AComA and/or PComP with accelerated and turbulent flow

- impaired cerebral vasomotor reactivity (CVR)

