ISCHEMIC STROKE / ETIOLOGY
Assessment and classification of atherosclerotic plaques
David Goldemund M.D.
Updated on 18/11/2023, published on 18/04/2023
Updated on 18/11/2023, published on 18/04/2023
Atherosclerosis
- atherosclerosis (AS) is a chronic, progressive systemic disease affecting the arterial wall that is a leading cause of death and disability in developed countries
- the disease involves the accumulation of lipids, calcium, and other blood components within the arterial wall
- these lesions, called plaques, can result in arterial stenosis and may be complicated (thrombosis, rupture, etc.)
- plaques are predominantly found in specific segments of large and medium-sized arteries (carotid and coronary arteries, thoracic and abdominal aorta, arteries of the circle of Willis, etc.). Segments with arterial branches have the highest affinity for atherosclerotic changes
- while the exact cause is unknown, numerous vascular risk factors contribute to the disease
- the disease involves the accumulation of lipids, calcium, and other blood components within the arterial wall
- plaques may either be asymptomatic or may cause cardiovascular events (such as coronary artery disease, stroke, peripheral artery disease, etc.) due to:
- progressive narrowing to complete arterial occlusion (symptoms vary depending on the quality of the collateral circulation)
- artery to artery embolisms
- combination of both mechanisms (embolism occurring at the time of ICA occlusion)

- atherosclerosis generally begins in young adulthood and progresses with age; the rate of progression is individual, but nearly everyone is affected to some degree by the age of 65
- modern imaging techniques allow a qualitative assessment of atherosclerotic plaque beyond mere measurement of the stenosis grade
- the first stage of atherosclerosis in the carotid arteries, detectable by sonography or MRI, is an increase in the intima-media thickness (IMT) (classified as a type 3 lesion according to AHA)

Atherosclerotic plaques classification

Endothelial dysfunction
- microscopic changes
Fatty streaks
- yellow streaks that do not extend into the lumen of the artery
- formed by foam cells
Fibroatheroma
- well-defined, stiff, pale grey or yellow deposits in the vessel wall (the color depends on the fat content)
- fibroatheroma protrudes into the lumen and causes its narrowing
- it may lack the lipid core and exhibit heavy calcifications
Complicated lesions
- complex plaques with lipid core with either surface defect, hemorrhage, or thrombus
| Type I |
|
| Type II |
|
| Type III |
|
| Type IV |
|
| Type V |
|
| Va |
|
| Vb |
|
| Vc |
|
| Type VI |
|
| Ultrasound evaluation of atherosclerotic plaques | ||
| Atherosclerotic (AS) plaque is defined as a lesion ≥ 1.5 mm on cross-section; lesions < 1.5 mm are classified as enlarged intima-media thickness (IMT) |
||
Echogenicity
|
 |
|
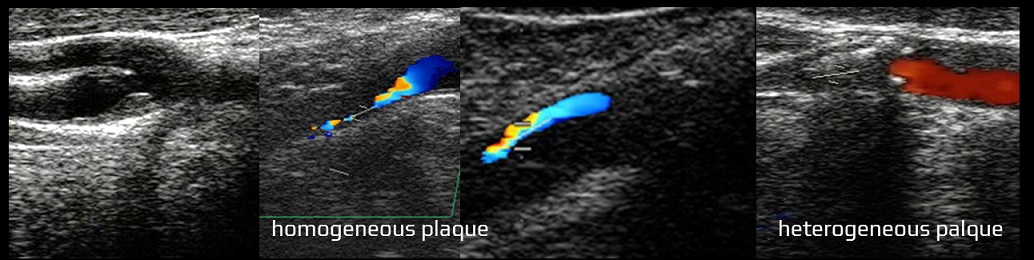
Homogeneity
|
 |
|
Surface
|
  |
|
| Gray-Weale classification of plaque echogenicity |
|
| Type I – hypoechogenic plaque Type II – predominantly hypoechogenic plaque with hyperechogenic areas Type III – predominantly hyperechogenic plaque with small hypoechogenic foci Type IV – homogeneous hyperechogenic plaques |
- each plaque can be characterized by:
- size (length and width)
- shape (circular, semicircular, eccentric)
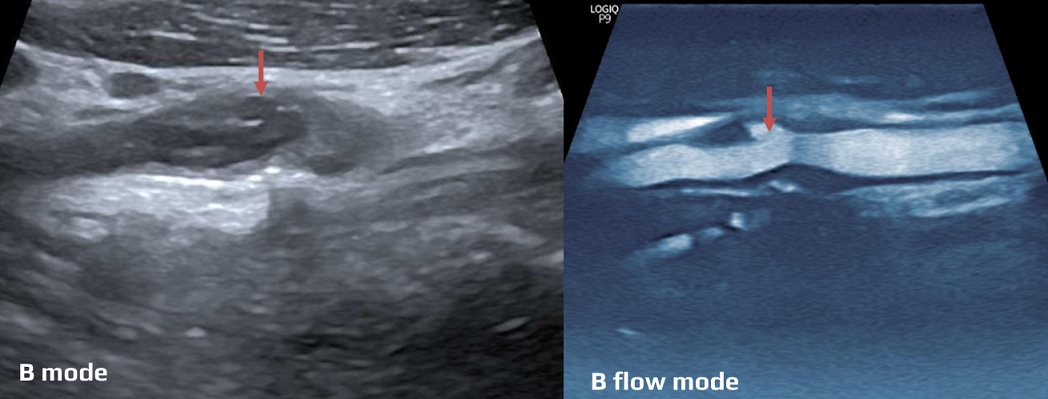
- surface (smooth, rough, exulcerated)
- density (hypodense, isodense, hyperdense)
- homogeneity (homogeneous x heterogeneous)
- presence of calcifications and intraluminal thrombi (ILT)
- the presence of ILT or ulcers increases the likelihood of symptomatic stenosis
- smooth or heavily calcified plaques are associated with a relatively low risk of cardiovascular events [Eesa, 2010]
- in the case of extensive calcifications, CTA (with an adjusted window) outperforms ultrasound, which must rely on Doppler examination (B-mode and color mode are usually inconclusive due to acoustic shadows)





| AHA classification | MRI classification |
| Type I: initial lesion with foam cells (endothelial dysfunction) | Type I-II: near-normal wall thickness, no calcification |
| Type II: fatty streak | |
| Type III: preatheroma with extracellular lipid pools | Type III: diffuse intimal thickening or small eccentric plaque with a small lipid core, no calcification |
| Type IV: atheroma with a confluent extracellular lipid core | Type IV-Va: plaque with lipid or necrotic core surrounded by fibrous tissue with calcium |
| Type Va: fibroatheroma | |
| Type Vb: plaque with lipid core or fibrotic tissue, large calcifications (also type VII) |
Type Vb: plaque with a lipid core or fibrous tissue, large calcifications |
| Type Vc: plaque with large fibrotic tissue, no lipid core (also type VIII) |
Type Vc: plaque with fibrous tissue, no lipid core |
| Type VI: complex plaque (with hemorrhage and/or thrombus) |
Type VI: complex plaque with hemorrhage or thrombus |
| MRI findings of the plaque components | ||||
| TOF | T1 | T2 | T1-enhanced | |
| Fibrous tissue | iso/hypo | iso | hyper | + |
| Lipid-rich | iso | iso/hyper | hypo | – |
| Calcification | hypo | hypo | hypo | – |
| Hemorrhage | hyper | hyper | variable | – |
 on T1W")
Stable plaque
- low lipid content
- minima tendency to rupture or thrombosis (usually Vb and Vc lesions according to AHA classification)
Unstable (high-risk) plaque
- mostly type Va and VI lesions (according to AHA classification)
- associated with a high risk of CV events
- exulcerated plaque [Kuk, 2014][Kanber, 2013]
- plaque with high lipid content
- plaque with necrotic core and fibrous cap
- plaque with a mobile component

- plaque with intraplaque hemorrhage (IPH)

- plaque with ↑angiogenesis [Vicenzini, 2012] [Saito, 2014] [Hiyama, 2010]
- dynamic contrast-enhanced MRI

- contrast-enhanced carotid ultrasound

- dynamic contrast-enhanced MRI