NEUROIMAGING / NEUROSONOLOGY
Subclavian (vertebral) steal syndrome
David Goldemund M.D.
Updated on 16/03/2024, published on 13/05/2023
Updated on 16/03/2024, published on 13/05/2023
- steal syndrome (or phenomenon), in general, is a phenomenon where blood flow is redirected (“stolen”) from one area to another, typically due to collateral circulation or the presence of a high-flow A-V shunt
- subclavian steal syndrome, also known as subclavian-vertebral artery steal syndrome, refers to an altered (usually retrograde) blood flow in the vertebral artery (VA) or the internal thoracic artery (ITA) due to a proximal stenosis/occlusion of the subclavian artery (SA) or brachiocephalic trunk (BCT)
- the upper extremity then receives blood from the vertebral artery at the expense of the posterior circulation
- subclavian steal is mostly asymptomatic and does not necessitate invasive evaluation or intervention
- a coronary variant may occur as an adverse effect of coronary artery bypass grafting (CABG) when the internal thoracic (also known as mammary) artery is used on the side of the stenotic/occluded subclavian artery
- dialysis access steal syndrome – altered blood flow to the hand in patients who have arteriovenous fistulas or grafts for hemodialysis
- the diagnosis of subclavian steal syndrome should be considered in patients who present with paroxysmal neurologic symptoms related to vertebrobasilar circulation and who have an upper extremity blood pressure difference; suspicion is increased if these episodes are provoked by the exercise of the affected extremity
- subclavian steal phenomenon affects the left side much more commonly than the right; if the left vertebral artery arises directly from the aortic arch (~ 2%), stenosis of the proximal left subclavian artery cannot cause the steal syndrome
Steal phenomenon vs. steal syndrome
- it is essential to distinguish between the subclavian steal phenomenon (an asymptomatic, incidental finding of altered flow in the VA) and subclavian steal syndrome (steal phenomenon + clinical signs and symptoms related to the compromised blood supply to the upper extremity or posterior circulation)
- the majority of patients with the steal phenomenon remain clinically asymptomatic
Pathophysiology
Subclavian steal syndrome
- vertebral artery steal syndrome is caused by stenosis or occlusion of the subclavian artery (SA) proximal to the origin of the vertebral artery or brachiocephalic trunk


- steal represents collateral flow from the brain into the territory of the subclavian artery
- flow alterations in the vertebral artery depend on the degree of SA stenosis
- clinical presentation is influenced by the quality of the intracranial collateral circulation
- symptomatic patients (with a steal syndrome) typically have poor collateral circulation and/or coexisting stenoses in the intra- or extracranial cerebral circulation
| Content available only for logged-in subscribers (registration will be available soon) |
Double steal phenomenon (carotid and vertebral)
- can be observed in patients with severe stenosis of the brachiocephalic trunk (BCT); flow is altered in both ipsilateral vertebral and carotid artery (the VA and ICA usually have a higher degree of steal than the common carotid artery)

Coronary-subclavian steal syndrome
- the internal thoracic (mammary) artery (ITA) supplies the anterior chest wall and the breasts
- if ITA is used in coronary artery bypass graft (CABG) surgery, stenosis or occlusion in the subclavian artery may lead to cardiac steal syndrome with angina symptoms
- during CABG, the distal end of the ITA is diverted to one of the coronary arteries
- subclavian artery stenosis must be excluded before proceeding with CABG!
Spinal artery steal syndrome
- vertebral artery flow reversal very rarely leads to hypoperfusion in the territory of the anterior spinal artery (ASA) (Mohassel, 2013)
Etiology
- atherosclerosis (the most common cause)

- more frequent on the left side (~ 80%)
- stenosis of the subclavian artery or brachiocephalic trunk (innominate artery) may cause less frequent steal on the right side
- typical vascular risk factors are present
- other vascular causes
- external compression of a subclavian artery caused by the cervical rib or scalene muscles (Thoracic Outlet Syndrome – TOS)
- steal is rare because the arterial compression is usually distal to the origin of the vertebral artery
- Takayasu arteritis

- typically in Asia
- radiation-induced vasculopathy
- iatrogenic lesion
- following surgical repair of congenital malformations (e.g., preductal coarctation of the aorta) or aortic dissection
- congenital anomalies
- A-V shunt (in dialysis individuals)
- may cause symptoms of steal in case of unrecognized SA stenosis
- accelerated flow may mimic subclavian artery stenosis (check flow in distal segments of the SA)
- external compression of a subclavian artery caused by the cervical rib or scalene muscles (Thoracic Outlet Syndrome – TOS)
Clinical presentation
- most commonly asymptomatic condition
- peripheral signs and symptoms (related to circulation issues in the upper extremity)
- weak/absent radial and ulnar pulses
- a difference in blood pressure between arms (lower on the affected side, typically with a difference of > 15-20 mmHg)
- arm claudication (rarely) – pain or fatigue in the arm occurs following exercise
- subclavian bruit may be audible
- cerebral signs and symptoms (often provoked by the physical exercise involving the affected arm)
- presyncope/syncope
- vertigo
- neurologic deficits form posterior circulation (ataxia, diplopia, visual field disorders, dysarthria, weakness/sensory disturbances)
- drop attacks
Diagnostic evaluation
- neurosonology (carotid duplex ultrasound + TCCD) is used as the initial study in patients with suspected subclavian steal (a blood pressure difference in the upper extremity, specific cerebrovascular symptoms)
- steal phenomenon is most commonly an incidental finding during carotid evaluation and a conservative approach is recommended in such cases
- vascular imaging (CTA/MRA/DSA) is added to confirm the vascular lesion if intervention is being considered

Neurosonology
- neurosonology serves as a baseline vascular imaging
- subclavian artery peak systolic velocity >240 cm/s predicts a significant subclavian artery stenosis
- visibility of the proximal segment of the subclavian artery is limited
- significant SA stenosis is associated with altered flow in the vertebral artery
- hemodynamic changes in the VA can be categorized into the following stages:
- presteal (latent steal) – grade 1, Doppler shows systolic deceleration of flow with a split in the systolic part of the curve and reduced pulsatility
- incomplete steal – grade 2, biphasic flow with retrograde systole
- complete steal – grade 3, retrograde flow with increased resistance
- always assess the V4 segment and basilar artery (BA) using TCCD in addition to the extracranial portion of the VA


- patients with antegrade flow in the BA are less likely to experience symptoms
- upper limb compression or stress test – in all stages of the steal phenomenon, the altered flow pattern may become more pronounced after the release of compression or post-exercise
- examining the brachial artery is helpful – the flow distal to the subclavian stenosis is blunted with loss of the triphasic curve

 steal on Doppler ultrasound")
")

THE STEAL PHENOMENON IN A PATIENT WITH RIGHT SUBCLAVIAN ARTERY STENOSIS

Stenotic turbulent flow in the subclavian artery Incomplete steal phenomenon with biphasic flow in basilar artery Retrograde flow in V2 segment of the right vertebral artery

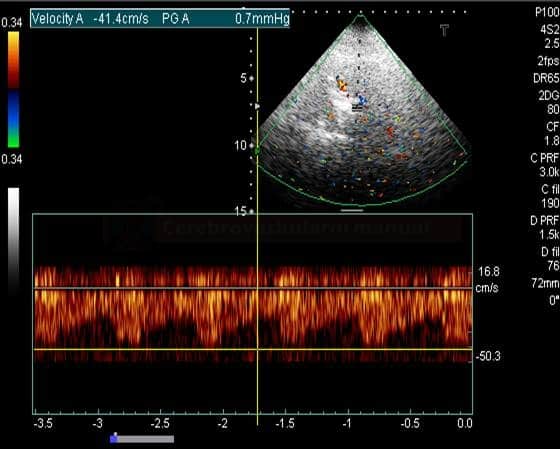 Anterograde flow in the V4 segment of the left vertebral artery
Anterograde flow in the V4 segment of the left vertebral artery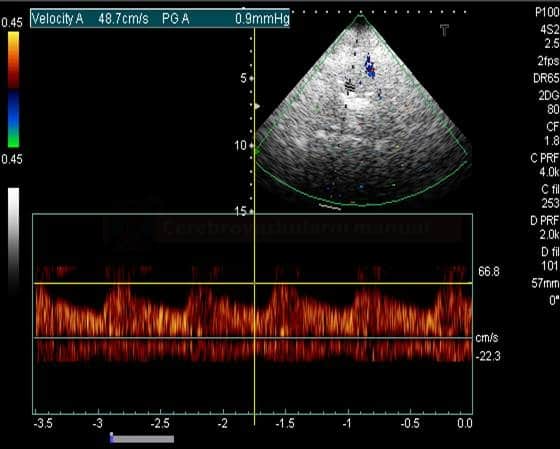 Retrograde flow in the V4 segment of the right vertebral artery
Retrograde flow in the V4 segment of the right vertebral artery



CT angiography
- direct detection of stenosis/occlusion in the subclavian artery (SA), brachiocephalic trunk (BCT), and other arteries (extra- and intracranial)

- provides precise measurement of the severity of stenosis and may show concurrent pathology involving the extracranial and intracranial arteries (aneurysm, thrombus, other stenoses)
- can distinguish atherosclerosis from other causes (such as vasculitis, compression, external compression, etc.)
- can not evaluate the hemodynamic consequences in the posterior circulation
- delayed filling of the ipsilateral vertebral artery can be observed, but the direction of flow cannot be determined – neurosonology is ideal for this task
MR angiography
- contrast-enhanced MRA (CE-MRA) can be used instead of CTA
- a technique that uses 3D spoiled gradient-echo (GE) sequences, with the administration of gadolinium-based contrast agents (GBCA)
- MRA may help determine the direction of flow in the vertebral artery
- vessel is absent on the flow-sensitive, low-resolution TOF localizer but is present on subsequent CE-MRA (Sheehy, 2005)
- MRA has a general tendency to overestimate the degree of stenosis (it shows the speed of flowing protons) and may not differentiate tight stenosis from complete occlusion correctly
DSA
- detects subclavian artery stenosis + delayed retrograde filling of the ipsilateral vertebral artery when other arteries are injected
- assess the remaining arteries for concomitant pathology (aneurysm, stenosis, etc.)
- however, hemodynamic consequences are easier and safer to evaluate by neurosonology
 on DSA")
Differential diagnosis
- repetitive, stereotypical, transient episodes provoked by arm exercise are typical for vertebral steal syndrome
- posterior stroke requires complete etiological evaluation → Vertebrobasilar steno-occlusive disease
Management
Treatment should be highly individualized based on age, overall health, the severity of stenosis and symptoms
Conservative therapy
- the mainstay is treatment of the underlying cause (which is usually atherosclerosis)
- asymptomatic patients or those with minimal symptoms may be monitored (clinically and via ultrasound)
- most commonly, symptoms remain stable or improve over time without vascular intervention
- asymptomatic patients or those with minimal symptoms may be monitored (clinically and via ultrasound)
- aggressive management of traditional vascular risk factors + antiplatelet therapy
- blood pressure should be measured in both arms; BP management should be based on the values obtained in the unaffected arm; any increase in antihypertensive dosage must be carefully monitored (BP drop may worsen the steal)
- low-dose aspirin
- lipid-lowering drugs
- blood pressure should be measured in both arms; BP management should be based on the values obtained in the unaffected arm; any increase in antihypertensive dosage must be carefully monitored (BP drop may worsen the steal)
- lifestyle modifications (smoking cessation, regular exercise, and healthy diet)
- specific therapy of less common nonatherosclerotic etiologies is discussed separately (such as Takayasu arteritis)
Intervention
- most commonly reserved for severe symptomatic cases
- the type of intervention is selected based on the underlying etiology, the patient’s age and condition, the location of the lesion, and the patient-specific anatomy
- subclavian angioplasty with stenting
- usually the preferred method unless the origin of the vertebral artery is at risk
- premedication is the same as for carotid angioplasty and stenting
- bypass surgery
- carotid-subclavian bypass
- aorta-subclavian bypass
- subclavian angioplasty with stenting
- in the presence of concomitant symptomatic carotid disease, carotid endarterectomy should be offered first (improved flow after revascularization may alleviate potential subclavian steal symptoms)
